Your Weekly Checkup: Managing Atrial Fibrillation
“Your Weekly Checkup” is our online column by Dr. Douglas Zipes, an internationally acclaimed cardiologist, professor, author, inventor, and authority on pacing and electrophysiology. Dr. Zipes is also a contributor to The Saturday Evening Post print magazine. Subscribe to receive thoughtful articles, new fiction, health and wellness advice, and gems from our archive.
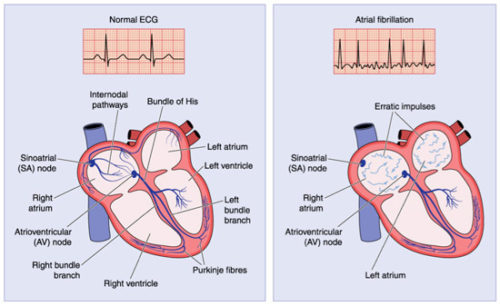
Your heart has four chambers: two on top called the atria, and two on the bottom called the ventricles. Fibrillation, a disorganized, rapid (400+/minute) heart rhythm, can occur in the atria (atrial fibrillation, AF) or the ventricles (ventricular fibrillation, VF). Since fibrillation prevents the heart from contracting and propelling blood forward, it is lethal when it occurs in the ventricles unless stopped by a shock within seconds to a few minutes. Ventricular fibrillation is responsible for a significant number of the 300,000 sudden deaths annually in the U.S.
Atrial fibrillation, on the other hand, is the most common sustained heart rhythm disorder, affecting over 5 million Americans, and expected to increase to more than 12 million by 2030. Though considered a fairly benign arrhythmia (abnormal heart rhythm) for many years, we now realize that AF can also be dangerous, although nowhere as lethal as VF. The incidence of AF increases with age and is associated with an increase of heart failure, sudden death, total mortality, and strokes. A recent study estimated that the lifetime risk for atrial fibrillation is approximately 37% after age 55 years.
Many environmental factors help explain why the incidence of this arrhythmia is approaching near epidemic proportions. Risk factors for developing AF include hypertension, obesity, heart attacks, excessive alcohol consumption, excessive physical training, smoking, stress, diabetes, heart failure, elevated LDL cholesterol, and (perhaps) sleep apnea. Appropriate lifestyle changes that address these risk factors can help reduce AF’s incidence.
Three clinical aspects of the arrhythmia require treatment:
- eliminating the AF and restoring a normal heart rhythm when possible
- controlling the heart rate of the lower chamber (ventricles) if AF persists
- providing anticoagulation to reduce the risk of stroke
Because of these challenging therapeutic decisions in treating AF patients, as well as the complexity of the arrhythmia, treatment may be best handled by a cardiologist in an urban setting. A recent study published in the Canadian Journal of Cardiology concluded that AF patients lived longer when cared for by cardiologists, while another study found that the chance of dying from AF was greater when patients were treated in rural compared with urban hospitals.
The take home message is that AF is frequent, particularly in older folks, and that treatment by skilled medical professionals can either eliminate it or treat it to make it quite compatible with a fairly normal life.