Your Weekly Checkup: Avoid the Holiday Heart Attack
“Your Weekly Checkup” is our online column by Dr. Douglas Zipes, an internationally acclaimed cardiologist, professor, author, inventor, and authority on pacing and electrophysiology. Dr. Zipes is also a contributor to The Saturday Evening Post print magazine. Subscribe to receive thoughtful articles, new fiction, health and wellness advice, and gems from our archive.
Order Dr. Zipes’ new book, Damn the Naysayers: A Doctor’s Memoir.
As we approach the holiday season, it is important to take stock of one’s health status. I have emphasized well known risk factors such as smoking, exercise, hypertension, diabetes, and diet. But what about less obvious variables, such as time of year and the impact of holidays?
Multiple studies have shown that mortality from a variety of causes including sudden cardiac deaths, suicides, homicides, and automobile fatalities increases during the winter months.
Explanations include the impact of cold weather, as well as behavioral changes that can involve travel, eating, drinking, exercising, working, and vacationing. Delay in seeking or finding competent medical attention while on holiday is also a potential reason. The short days of winter with overall reduced sunlight exposure may play a role.
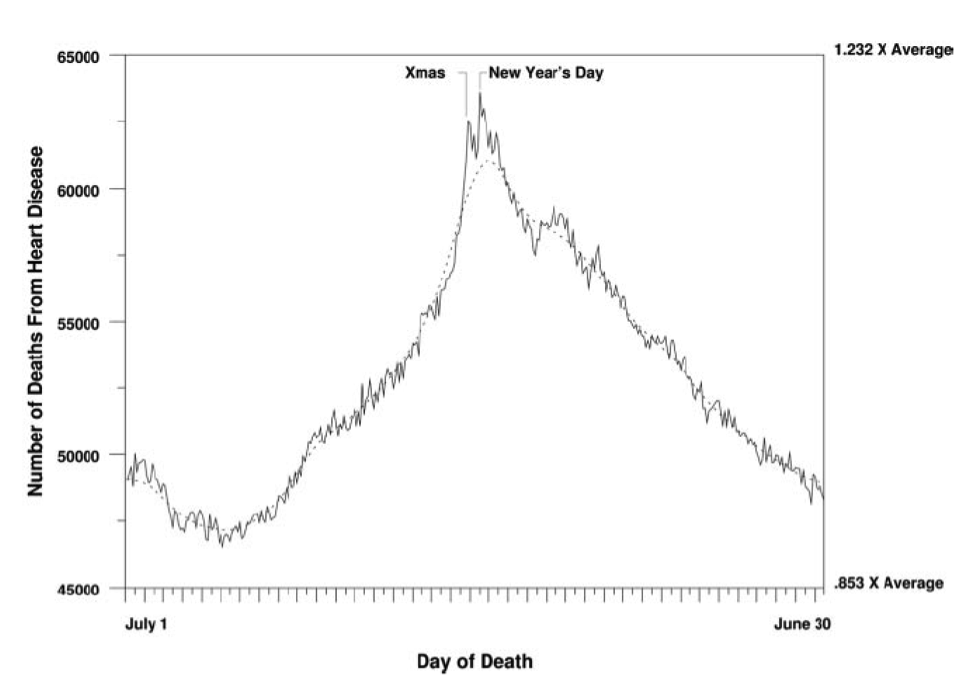
One study of cardiac deaths in Los Angeles found that deaths from coronary heart disease peaked around the holiday period of Christmas and the New Year, despite very little outdoor temperature change.
That observation raises the question whether the actual holidays play a role rather than the cold weather.
A study published almost fifteen years ago investigated whether distinct mortality peaks occurred during the Christmas and the New Year’s holidays. The researchers examined 53 million U.S. death certificates from 1973 through 2001 and noted that a spike in daily mortality of almost 5 percent occurred for both cardiac and noncardiac patients during the Christmas/New Year’s holiday period. As can be seen in the figure, the solid line indicates actual mortality while the interrupted line indicates the mortality that would have occurred without the holidays.
Another study published two years ago sought to eliminate the role played by winter’s cold weather by studying holiday deaths in New Zealand where the seasons are reversed compared to that of North America, so there it is summer in December. The researchers analyzed New Zealand mortality data for a 25-year period (1988-2013) and found evidence of a Christmas holiday effect with an excess event rate of 4.2 percent leading to about four additional deaths per annum (it’s a small country). The study also found that people who died from heart-related causes during Christmastime were slightly younger (76.8 years) than those who died of similar causes during the rest of the year.
It is clear that we can now add Christmas/New Year’s holidays as a risk factor for increased cardiac and noncardiac mortality.
But why? What are the causes?
Among the multiple potential explanations for this association, including overindulgence in holiday food and drink, as well as the emotional stress involved, is the possibility that the holidays induce delays in seeking necessary medical treatment. Sometimes people who are sick attempt to “hold on” until the holiday season is over and contribute to the twin holiday mortality spikes. Whatever the reason(s), cardiac and noncardiac deaths clearly surge during Christmas and the New Year.
The take home message for readers is advice I’ve given before: moderation in all things, including moderation. Add to that the admonition not to delay seeking medical help for new or worsening old symptoms — delays that could prove fatal.
Despite the increased risk, enjoy the holidays!
Your Weekly Checkup: Good News about Fish Oil Supplements
“Your Weekly Checkup” is our online column by Dr. Douglas Zipes, an internationally acclaimed cardiologist, professor, author, inventor, and authority on pacing and electrophysiology. Dr. Zipes is also a contributor to The Saturday Evening Post print magazine. Subscribe to receive thoughtful articles, new fiction, health and wellness advice, and gems from our archive.
Order Dr. Zipes’ new book, Damn the Naysayers: A Doctor’s Memoir.
Previous information about fish oil supplementation has been disappointing, showing conflicting or no cardiovascular benefits. However, results from a recently published study are going to upend that conclusion.
The New England Journal of Medicine published a study of a randomized trial of more than 8,000 patients that tested a proprietary fish oil compound called icosapent ethyl (Vascepa). Icosapent ethyl is a highly concentrated preparation of eicosapentaenoic acid, the critical omega-3 fatty acid ingredient in fish oil.
Enrolled patients were 45 years of age or older and had established cardiovascular disease, or were 50 years or older and had diabetes mellitus and at least one additional risk factor. They had a mean age of 64 years, almost 30 percent were women, and all had been receiving statin therapy, so they had a normal low-density lipoprotein (LDL or “bad” cholesterol) of 41 to 100 mg per deciliter.
However, they had an elevated fasting triglyceride level (135 to 499 mg per deciliter), which is a known independent risk factor for heart attacks and strokes.
Icosapent ethyl versus placebo significantly reduced major adverse cardiovascular (CV) events, including cardiovascular death, nonfatal heart attack, nonfatal stroke, coronary revascularization, or unstable angina, by 25%, over a median of almost five years. The risk of CV death alone was reduced by 20 percent. Triglycerides were reduced by almost 20 percent.
Several factors make this trial notable. Patients were already taking a statin and had LDL controlled, yet still had a significant reduction in CV events. The daily dose of icosapent ethyl was 4 grams, considerably more of the highly purified omega-3 formulation than in previous trials, which may account for differences from previous trials. Clear benefits took about a year to become evident and were present despite an increase in LDL from 76 to 84 mg/dL over 1 year. Finally, despite the reduction in CV events, the incidence of atrial fibrillation rose, and patients experienced slightly more bleeding events. Heart failure did not change.
The significantly lower risk of major adverse CV events with icosapent ethyl appeared to occur regardless of the patients’ triglyceride levels at 1 year. Therefore, the benefits of icosapent ethyl may not just be due to a reduction in triglycerides. Icosapent ethyl may also have anti-inflammatory, antioxidative, plaque-stabilizing properties.
The results of the study, called “Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia” (REDUCE-IT) should not be generalized to other fish oil preparations, especially those containing omega-3 fatty acid mixtures, which are variable and unregulated, and which have not been shown to have clinical benefit. Over-the-counter fish oil products generally contain 1,000 or 1,200 mg of fish oil but only about 300 mg that is actually eicosapentaenoic acid.
Two other recent omega-3 studies using a lower dose failed to reduce CV outcomes. In a study called “The Vitamin D and Omega-3 Trial” (VITAL) in which patients were given omega-3 fatty acid at a dose of 1 gram/day, the fish oil supplementation did not reduce the incidence of major CV events. Similarly, the “Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus” (ASCEND) trial of 1 gram/day of omega-3 fatty acid in 15,480 patients with diabetes without evidence of cardiovascular disease found no significant difference in the risk of serious vascular events between those who were assigned to receive omega-3 fatty acid supplementation and those who were assigned to receive a placebo.
Therefore, it is quite clear that the dose of omega-3 fatty acid is important, and that 4 grams/day has pronounced CV benefit, while 1 gram/day does not. It is exciting to think that a dietary supplement may be able to add CV benefits to statin drugs. Which patients, in addition to those with elevated triglyceride levels, should receive this new drug awaits further testing.
Your Weekly Checkup: Can You Be Fit and Fat?
We are pleased to bring you “Your Weekly Checkup,” a regular online column by Dr. Douglas Zipes, an internationally acclaimed cardiologist, professor, author, inventor, and authority on pacing and electrophysiology. Dr. Zipes is also a contributor to The Saturday Evening Post print magazine. Subscribe to receive thoughtful articles, new fiction, health and wellness advice, and gems from our archive.
Like many Americans, I am overweight—not a lot, but I’d love to lose ten pounds from my pot belly. Despite exercising an hour each morning, my weight remains constant because to lose, I must combine diet with exercise, and I don’t do the former. Because I lift weights and work out on the treadmill, bike, and elliptical, I tell myself I am fat but fit.
Is that really true? Can I be overweight and not at increased risk for heart disease? A recently published study based on the electronic health records of 3.5 million British patients followed from 1995 to 2015 says no. Being overweight makes me 30% more likely to develop coronary heart disease (atherosclerosis) compared with normal weight individuals, despite the absence of other health issues. The study outcome challenges the belief that I can be metabolically healthy (no diabetes, elevated cholesterol, or high blood pressure), overweight, and not at increased risk, possibly because obesity is associated with inflammation, and the latter plays a role in the development of coronary heart disease. They conclude that there is no such thing as benign obesity. Importantly, the authors also found that normal weight individuals who had metabolic risk factors such as diabetes were also at increased risk for developing coronary heart disease, despite not being overweight.
Critics argue that the study, despite its size, has flaws and that fitness outweighs fatness, if the latter is not excessive. This is a crucial point because many people, like me, find it easier to exercise daily than to diet. A bad combination is to be sedentary and overweight. Being fit at least counteracts some of the risk of being fat.
The same study found that being too lean also has risks. Underweight individuals with no metabolic abnormalities were at higher risk for stroke than individuals who were at normal weight, overweight, or obese with no metabolic problems. The risk to underweight people with metabolic issues increases even further. Metabolic health is important regardless of weight.
So, what should you do? Lose weight, of course. If you cannot, be sure to treat metabolic abnormalities such as controlling blood pressure, reducing cholesterol, and keeping blood sugar normal. This will counter some of the risk from being overweight. And get off the couch! Run, walk, exercise any way you want. But do something!